|Videos|April 7, 2022
Educated Patient® Multiple Myeloma Summit CAR/BiTE Presentation: March 12, 2022
Author(s)Ryan McDonald
Watch Dr. Sham Mailankody, from Memorial Sloan Kettering Cancer Center, discuss CAR and BiTE therapy, during the CURE Educated Patient Multiple Myeloma Summit.
Advertisement








Over the past year, the Food and Drug Administration (FDA) approved two CAR-T cell therapies for the treatment of relapsed or refractory multiple myeloma, developments that, according to one expert, represent the start of significant growth in the next several years.
“There are other potential immunologic approaches coming along, (such) as bi-specific antibodies (and) allogeneic CAR T cells,” Dr. Sham Mailankody, a medical oncologist and hematologist at Memorial Sloan Kettering Cancer Center in New York City, said during a recent CURE® Educated Patient® Summit on multiple myeloma.
“We’re only touching the surface of what's feasible with these treatments. As we make progress, we're going to look at combinations … at using these treatments earlier on for patients with high-risk myeloma, new diagnoses or early relapses. And hopefully we'll continue to build on this early success with these treatments.”
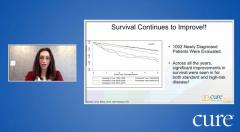
Great Progress
While Mailankody mostly discussed the recent developments of CAR-T cell therapies and highlighted the future of the myeloma space, he also noted that great progress has made in the treatment of this disease over the past several decades.
“When you get to 2000 and beyond, this is where we see a lot of these new drugs becoming available — proteasome inhibitors, immunomodulatory drugs (and) antibodies like (Darzalex [daratumumab]),” he said.
Collecting T Cells
Typically, Mailankody said during his presentation, T cells are collected from a patient’s body and then sent to a lab for processing. Once at the lab, the T cells are activated, transduced and expanded. This process, he noted, can take upwards of four weeks and possibly longer.
After the T cells are manufactured in the lab, they can then be stored until a patient with relapsed or refractory multiple myeloma can be administered the treatment. Prior to the redistribution of these manufactured CAR T cells, patients are often treated with low-intensity chemotherapy such as cyclophosphamide and fludarabine for several days.
The process to readminister the manufactured cells, according to Mailankody, can take upwards of an hour. The T cells are administered intravenously, similar to, he said, a blood transfusion. Patients are then monitored to not only identify if the treatment is working, but if they are developing any side effects such as low blood counts or negative effects on the nervous system.
To monitor any developments, Mailankody noted, patients are normally hospitalized for one to two weeks post infusion of the manufactured CAR T cells.
Targeting the BCMA Protein
The two recently FDA-approved CAR-T cell therapies — Abecma (idecabtagene vicleucel) and Carvykti (ciltacabtagene autoleucel) — target cells that express the B-cell maturation antigen, or BCMA.
Mailankody described it as the T cells are manufactured to target the BCMA protein, which is present in myeloma cells.
Both approvals, he noted, were based on data from large, multicenter trials. For Abecma, the study authors assessed the safety and efficacy of the agent in a trial of 127 patients with relapsed and refractory myeloma who were previously treated with at least three lines of therapy. Most patients in the study (72%) either partially or completely responded to the treatment, of whom 28% showed complete response to Abecma. This effect persisted for at least 12 months in 65% of these patients.
Carvykti was approved using findings from the CARTITUDE-1 clinical trial, which demonstrated that 98% of patients with pretreated relapsed/refractory myeloma responded to treatment with the study drug.
Patients in both trials, according to Mailankody, had triple-refractory disease, meaning their myeloma failed to respond to treatment with a proteasome inhibitor, immunomodulatory drug and a CD-38 antibody.
Ultimately, he noted, the data from these two trials show the effective use of novel CAR-T cell therapies in this patient population.
What’s Next?
The two FDA-approved CAR-T cell therapies are examples of autologous stem cell transplants, meaning T cells are taken directly from a patient, manufactured in a lab and transplanted back into said patient.
But one potential future option, he highlighted, is the use of allogeneic CAR T cells. In this instance, T cells would be harvested from a healthy donor and infused into a patient with multiple myeloma.
There are several benefits to this practice, according to Mailankody. For instance, providers could bulk manufacture T cells and store them for usage at any time. This means that patients theoretically would not need to receive bridge therapies — or treatments to mitigate the effects of the myeloma — while their own T cells are in the lab.
However, there are some concerns. Mailankody stressed that the use of donor T cells could lead to graft-versus-host-disease, which means that the donor’s T cells may negatively react to the recipient’s existing tissues. Another challenge, he expressed, is the opposite, or host-versus-graft disease. This side effect occurs when the recipient’s immune system attacks, or rejects, the donor’s T cells.
“Therefore, (this) disallows the T cell from doing (its) job (and) prevents the T cells from expanding and going after BCMA-positive cells,” he said.
There are, however, several pharmaceutical companies designing specific treatments to ensure few occurrences of either graft-versus-host-disease or host-versus-graft-disease.
BCMA Isn’t the Only Target
Although Mailankody noted that there has been significant interest in targeting BCMA — take Abecma and Carvykti for example — researchers are constantly identifying and assessing treatments for other targets such as CD38 and SLAMF7.
He said that at Memorial Sloan Kettering Cancer Center, researchers have been highly focused on targeting GPRC5D.
In a small study of 16 patients, the use of MCARH109 — a GPRC5D-directed CAR-T cell therapy — induced at least a partial response in 69% of patients at the time of data reporting. Moreover, of those patients, 25% had a complete response to treatment.
Notably, he said, 10 of the patients had previously received treatment that targeted BCMA. In these patients, eight responded to treatment with MCARH109. Additionally, of the eight patients who were treated with previous CAR T cells, 75% responded to this GPRC5D-directed CAR-T cell therapy.
“(This suggests) that this is an effective option possibly for patients with previous CAR T cells,” he said. “CAR T cells after CAR T cells is possible, particularly with a different target, here in this case, patients got a BCMA CAR-T cell therapy, did well for a while and then they progressed … and then had another good response to the second CAR T cell as well.”
For more news on cancer updates, research and education, don’t forget to
Advertisement
Related Content





Advertisement
Advertisement
Trending on CURE
1
FDA Updates Safety Warnings for Common Chemotherapy Drugs
2
FDA Removes Use Limitation for Yescarta in Primary CNS Lymphoma
3
KTX-1001 Elicits Responses in Some With Multiple Myeloma
4
Real-World Data with Amtagvi Show High Response Rates in Advanced Melanoma
5